Volume 14, Number 6—June 2008
Letter
Splenic Rupture and Malignant Mediterranean Spotted Fever
Figure
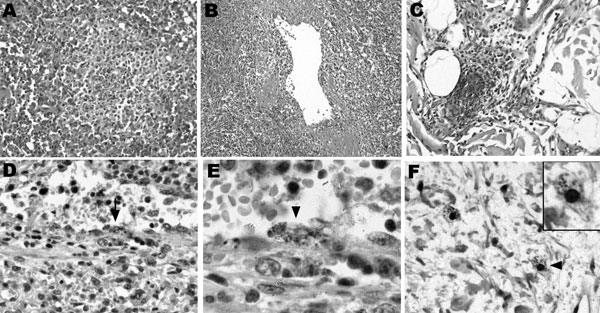
Figure. Histopathologic and immunohistochemical labelings of spleen and skin tissue samples. Tissue samples were fixed in 10% formalin, paraffin-embedded, and examined after hematoxylin-eosin staining, Gimenez staining, or immunostaining with the R47 anti-Rickettsia conorii polyclonal rabbit antibody. The spleen red pulp indicated congestion and ill-defined nodules varying in size and comprising macrophages, polymorphonuclear neutrophils, and necrotic cells (A, magnification ×100). A diffuse macrophage infiltration with abundant hemophagocytosis (not shown) and venulitis (B, magnification ×50) was also observed. In the skin, leukocytoclastic vasculitis with focal vascular necrosis and nonocclusive luminal thrombi were noted in dermal capillaries (C, magnification ×100). Intracellular images evocative of rickettsiae were observed in the splenic arteriolar endothelium upon immunohistochemical staining (D, arrow, magnification ×200; magnified view shown in E, arrowhead, magnification ×500). No infected cells were observed in nodular inflammatory splenic lesions. Immunohistochemical staining also disclosed intracellular immunolabeled dots in cells that could correspond to infected dermal macrophages (F, arrowhead, magnification ×300; magnified view shown in inset, magnification ×600), at a distance from the vascular alterations. Endothelial cells of dermal capillaries were also immunolabeled (Appendix Figure).