Volume 21, Number 6—June 2015
Letter
Klebsiella pneumoniae Co-Producing NDM-5 and OXA-181 Carbapenemases, South Korea
To the Editor: Carbapenemase-producing Enterobacteriaceae are being reported worldwide. Travel, medical tourism, and cross-border transfer of patients might play a role in the spread of these bacteria (1,2). Klebsiella pneumoniae co-producing New Delhi metallo-β-lactamase 5 (NDM-5) and oxacillinase 181 (OXA-181) carbapenemases was detected in South Korea in 2014.
On April 13, a 75-year-old man who had had a cerebral infarction was transferred from a tertiary care hospital in Abu Dhabi, United Arab Emirates (UAE), to Samsung Medical Center (Seoul, South Korea) for rehabilitation therapy. In Abu Dhabi, he had received broad-spectrum antimicrobial drugs for aspiration pneumonia. While at Samsung Medical Center, he experienced septic shock and acute respiratory failure due to pneumonia and was transferred to the medical intensive care unit (ICU). Carbapenem-resistant K. pneumoniae (strain CC1409-1) was isolated from a culture of bronchoalveolar lavage fluid. He was given meropenem and colistin for treatment of pneumonia, was discharged, and returned to the UAE.
Four months later, carbapenem-resistant K. pneumoniae (strain CC1410-1) was identified in the tracheal aspirate of a 74-year-old woman admitted to the surgical ICU at Samsung Medical Center for traumatic intracranial hemorrhage. She had no underlying disease or previous history of hospitalization or travel abroad. She was given colistin and piperacillin/tazobactam. Following the identification of colistin resistance, colistin was switched to tigecycline. However, her clinical condition worsened (aggravated pneumonia), and she died of refractory respiratory failure.
In vitro antimicrobial drug susceptibility tests of 2 isolates were performed by using broth microdilution. Results were interpreted following Clinical and Laboratory Standards Institute guidelines (3), except for those for colistin and tigecycline, for which European Committee on Antimicrobial Susceptibility Testing breakpoints were used (4). The first isolate was susceptible to colistin but none of the other antimicrobial agents tested (cefepime, ceftriaxone, ceftazidime, aztreonam, amikacin, ciprofloxacin, trimethoprim/sulfamethoxazole, ertapenem, imipenem, and meropenem)whereas the second isolate was susceptible only to tigecycline. Modified Hodge tests for both isolates showed positive results. Production of metallo-β-lactamase was detected by an imipenem-EDTA double-disk synergy test.
The presence of carbapenemase genes was determined by PCR and DNA sequencing (2). The blaNDM and blaOXA-48 genes were detected in both isolates. The PCR product sequences were consistent with those of NDM-5 (GenBank accession no. JN104597.1) and OXA-181 (GenBank accession no. JN205800.1). Further analyses for other β-lactamases (TEM-type, SHV-type, and CTX-type) and 16S rRNA methylase aminoglycoside resistance determinants (armA, rmtA, rmtB, rmtC, rmtD, rmtF, and npmA) revealed that both isolates carried blaTEM-1, blaSHV-11, blaCTX-M-15, and rmtB genes.
Figure
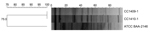
Figure. Dendrogram of pulsed-field gel electrophoresis patterns showing the genetic relationship between 2 Klebsiella pneumoniae isolates co-producing New Delhi metallo-β-lactamase 5 and oxacillinase 181 carbapenemases, South Korea, 2014. ATCC BAA-2146 indicates New...
Clonal relatedness was investigated by using multilocus sequence typing and pulsed-field gel electrophoresis (PFGE) (5,6). Multilocus sequence typing revealed that both isolates belonged to sequence type 147. PFGE showed that both isolates were the same strain (Figure).
The 2 patients were never hospitalized in the same ward and there was a substantial time lag between their hospitalizations. However, given sequence type and PFGE patterns between 2 isolates, we suspected nosocomial cross-transmission and performed infection control measures, including strict contact precautions and enhanced environmental cleaning with daily monitoring in the surgical ICU. In addition, environmental cultures and active surveillance cultures (rectal swabs and respiratory samples) on all patients in the units where these isolates were identified were performed to find asymptomatic carriers or contaminated environments as potential sources of transmission. All samples tested were negative for carbapenemase-producing Enterobacteriaceae. No further cases were reported in the hospital.
NDM-5 was first identified in a multidrug-resistant Escherichia coli sequence type 648 isolate from a patient in the United Kingdom who had a recent history of hospitalization in India (7). NDM-5 differs from existing enzymes due to substitutions at positions 88 (Val→Leu) and 154 (Met→Leu). OXA-181, a variant of OXA-48, was initially reported in India but has been sporadically detected in the United Kingdom, the Netherlands, France, New Zealand, Oman, and Singapore (8). It has also been found to be associated with other carbapenemase genes, such as the blaNDM-1 and blaVIM-5 genes, and particularly in isolates with a link to the Indian subcontinent.
In the cases we describe, the first K. pneumoniae isolate was recovered from a patient transferred from the UAE. Recent studies suggest that the Middle East, a region with close ties to the Indian subcontinent that hosts a large expatriate population, may act as another reservoir of OXA-48 and NDM producers (9,10). The emergence of extremely drug-resistant isolates carrying multiple carbapenemase genes is of concern because of limited treatment options and the possibility of global dissemination by means of cross-border transfer. A collaborative interdisciplinary strategy, including active surveillance for high-risk patients and adequate infection control measures against spread of such highly transmissible multidrug-resistant strains in health care settings, is necessary.
References
- Cantón R, Akóva M, Carmeli Y, Giske CG, Glupczynski Y, Gniadkowski M, Rapid evolution and spread of carbapenemases among Enterobacteriaceae in Europe. Clin Microbiol Infect. 2012;18:413–31. DOIPubMedGoogle Scholar
- Nordmann P, Naas T, Poirel L. Global spread of carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis. 2011;17:1791–8. DOIPubMedGoogle Scholar
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. Twenty-fourth informational supplement. M100-S24. Wayne (PA): The Institute; 2014.
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Clinical Breakpoints version 3.0. EUCAST; 2013 [cited 2015 Jan 8]. http://www.eucast.org/clinical_breakpoints/
- Diancourt L, Passet V, Verhoef J, Grimont PA, Brisse S. Multilocus sequence typing of Klebsiella pneumoniae nosocomial isolates. J Clin Microbiol. 2005;43:4178–82. DOIPubMedGoogle Scholar
- Matushek MG, Bonten MJ, Hayden MK. Rapid preparation of bacterial DNA for pulsed-field gel electrophoresis. J Clin Microbiol. 1996;34:2598–600.PubMedGoogle Scholar
- Hornsey M, Phee L, Wareham DW. A novel variant, NDM-5, of the New Delhi metallo-β-lactamase in a multidrug-resistant Escherichia coli ST648 isolate recovered from a patient in the United Kingdom. Antimicrob Agents Chemother. 2011;55:5952–4. DOIPubMedGoogle Scholar
- Poirel L, Potron A, Nordmann P. OXA-48-like carbapenemases: the phantom menace. J Antimicrob Chemother. 2012;67:1597–606. DOIPubMedGoogle Scholar
- Zowawi HM, Sartor AL, Balkhy HH, Walsh TR, Al Johani SM, AlJindan RY, Molecular characterization of carbapenemase-producing Escherichia coli and Klebsiella pneumoniae in the countries of the Gulf cooperation council: dominance of OXA-48 and NDM producers. Antimicrob Agents Chemother. 2014;58:3085–90. DOIPubMedGoogle Scholar
- Sonnevend A, Al Baloushi A, Ghazawi A, Hashmey R, Girgis S, Hamadeh MB, Emergence and spread of NDM-1 producer Enterobacteriaceae with contribution of IncX3 plasmids in the United Arab Emirates. J Med Microbiol. 2013;62:1044–50. DOIPubMedGoogle Scholar
Figure
Cite This Article1These authors contributed equally to this article.
Related Links
Table of Contents – Volume 21, Number 6—June 2015
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Doo Ryeon Chung, Division of Infectious Diseases, Samsung Medical Center, Sungkyunkwan University School of Medicine, Irwon-ro 81, Gangnam-gu, Seoul 135-710, South Korea
Top