Volume 21, Number 7—July 2015
Research
Results from the National Legionella Outbreak Detection Program, the Netherlands, 2002–2012
Abstract
In 2002, the National Legionella Outbreak Detection Program was implemented in the Netherlands to detect and eliminate potential sources of organisms that cause Legionnaires’ disease (LD). During 2002–2012, a total of 1,991 patients with LD were reported, and 1,484 source investigations were performed. Of those sources investigated, 24.7% were positive for Legionella spp. For 266 patients with LD, 105 cluster locations were identified. A genotype match was made between a strain detected in 41 patients and a strain from a source location. Despite the systematic approach used by the program, most sources of LD infections during 2002–2012 remained undiscovered. Explorative studies are needed to identify yet undiscovered reservoirs and transmission routes for Legionella bacteria, and improved laboratory techniques are needed to detect Legionella spp. in samples with a high background of microbial flora (such as soil).
Legionnaires’ disease (LD) is an acute pneumonia characterized by clinical symptoms and signs (e.g., cough, fever, lung infiltration observed on a chest radiograph) similar to those of pneumonias resulting from other pathogens. LD is caused by infection with Legionella spp. bacteria, which are most often transmitted to persons through inhalation of bacteria disseminated into the air as an aerosol from natural or man-made sources of water (1). The incubation period is 2–14 days. LD is thought to account for 2%–20% of all community-acquired pneumonias (2) and is fatal in ≈6%–11% of cases (3,4).
After a large outbreak of LD at a flower show in Bovenkarspel, the Netherlands, in 1999 (5), prevention and control of Legionella spp. infections became a national concern in the Netherlands, and legislation to prevent Legionella spp. in drinking water systems was introduced (6,7). This legislation obligated owners of aerosol-producing devices (e.g., shower heads and whirlpools), if third parties may be exposed to them, to conduct a risk analysis, develop a control plan, keep logs of control measures, and perform regular sampling for Legionella spp. contamination. In addition, in 2002, a National Legionella Outbreak Detection Program (NLODP) was implemented (8) on the basis of a report that LD outbreaks are often preceded and followed by small clusters of solitary cases (9). The aims of NLODP are early detection of small clusters of cases, identification of sources of infection, and implementation of early control measures to prevent additional LD cases or an outbreak. For evaluation of transmission pathways, infection sources are sampled, and genotypes of Legionella strains found in these samples are compared with those of clinical isolate(s) from the patient(s) associated with that source. To evaluate the findings of the NLODP during 2002–2012, we analyzed data to determine whether extensive investigation efforts could detect Legionella spp. in collected samples and conclusively identify environmental sources.
Patients
LD has been notifiable in the Netherlands since 1987. A case of LD is defined as laboratory-confirmed infection in a person having symptoms compatible with pneumonia or radiologic signs of infiltration. Laboratory evidence may be >1 of the following: isolation of Legionella spp. from respiratory secretions or lung tissue, detection of L. pneumophila antigen in urine, seroconversion or a >4-fold rise in antibody titers to L. pneumophila in paired acute- and convalescent-phase serum samples, a high antibody titer to L. pneumophila in a single serum sample, and direct fluorescent antibody staining of the organism or detection of Legionella DNA by PCR in respiratory secretions or lung tissue. In the Netherlands, microbiologic laboratories involved in the diagnosis and treatment of patients with pneumonia are requested to send available clinical isolates of Legionella spp. to the Legionella Source Identification Unit (LSIU), a part of the NLODP. LD cases in persons who had been outside the country for >5 of 9 days before disease onset were defined as nondomestic cases and excluded from the analyses. Cases in persons who stayed in a hospital or other health care setting (e.g., nursing home or rehabilitation center) for >1 day during the 2–14 days before symptom onset were defined as nosocomial cases.
Source Identification and Cluster Detection
Potential sources of infection were identified by Municipal Health Services (MHS) public health physicians and nurses, who used a standardized questionnaire to interview patients or relatives (Technical Appendix 1). The interview focused on tracking each patient’s exposure to potential sources of infection during the 2–14 days before symptom onset. All potential sources of infection were recorded in a database by the LSIU and used to identify clusters of LD cases by location and date. Each new LD case in this database was examined to determine if reported potential sources were linked to other LD cases. Because outbreaks of Legionnaires’ disease are often preceded and followed by small clusters of solitary cases (9), an arbitrary cluster definition was constructed that defined 2 types of clusters: location and geographic. A location cluster, which may represent a local contamination, was defined as cases reported within 2 years of each other in >2 persons who were reported to have been exposed to the same potential source of infection during the 2–14 days before symptom onset. A geographic cluster was defined as cases in >3 persons who lived <1 km apart and whose infections were reported within 6 months of each other. The concept of a geographic cluster was constructed to identify sources that patients were exposed to but unaware of (e.g., cooling towers). Patients could belong to >1 cluster. Data from the location cluster of the LD outbreak in Amsterdam in 2006 (7) were excluded from our analyses.
Sampling Procedure
As part of the NLODP, the LSIU is available to each MHS to collect samples from potential sources of Legionella infection for reported domestic LD cases. During 2002–2006, all identified potential sources of infection were investigated. However, because of budgetary reasons, after June 1, 2006, potential sources were investigated only if >1 of 4 sampling criteria was met: 1) a patient-derived isolate of Legionella spp. (from respiratory secretions or lung tissue) was available; 2) a location cluster was identified; 3) a geographic cluster was identified; or 4) the patient had stayed in a hospital or other health care setting during the incubation period. For geographic clusters, efforts were focused on identifying yet undiscovered potential sources (e.g., cooling towers near patients’ residences). If >1 of the 4 sampling criteria was met, trained LSIU laboratory staff collected water and swab samples from identified potential sources when possible. For each location, sampling points were selected by LSIU staff in cooperation with the facility’s technical team (when a team is available), and a comprehensive collection of water and swab samples was obtained from that location for further analysis.
Laboratory Investigations
Samples collected during the source investigation were analyzed for the presence of Legionella spp. (for an extensive description, see Technical Appendix 2). All L. pneumophila serogroup 1 (SG1) strains (clinical and environmental) were subsequently genotyped by sequence-based typing, as recommended by the ESCMID Study Group for Legionella Infections (10–12), and further determined by using the Dresden panel of monoclonal antibodies (13). The sequence-based typing profiles of the patient isolates were compared with those of the environmental strains found in samples of potential sources.
Statistical Analyses
Comparisons were made by using independent samples t-tests, nonparametric Mann-Whitney U-test, 2-tailed χ2 tests (proportions), and linear regression analyses (trends over time). All analyses were performed with PASW Statistics 8.0 (SPSS Inc., Chicago, IL, USA).
Patients
Figure
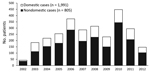
Figure. Legionnaires’ disease cases reported in the Netherlands, August 1, 2002–August 1, 2012. A total of 2,796 cases were reported; LD cases in persons who had been outside the country for <>
During August 2002–August 2012, a total of 2,796 LD cases were reported in the Netherlands, 805 (28.8%) of which were nondomestic (Figure). These travel-associated cases were excluded from the analyses, resulting in 1,991 reported possible domestic LD cases (mean of 193 [SD 76] cases annually); 119 (6.0%) of these were characterized as nosocomial cases. Most patients (72%) for this period were male (Table 1). The median age of reported case-patients increased from 55.3 (range 26.4–78.3) years in 2002 to 62.5 (range 27.0–91.6) years in 2012 (Table 1; linear regression, p trend <0.001).
Diagnostic Tests
The 1,991 LD cases were ascertained by 2,541 diagnostic tests (Table 2). Most cases were diagnosed by using urinary antigen tests (83.2%) or cultures (23.1%). Nosocomial LD cases (n = 119) were more often diagnosed by culture compared with community-acquired cases (37.0% vs. 22.2%; Pearson χ2 test, p<0.001). Nosocomial cases were more evenly distributed among male and female patients than were community-acquired cases (52.9% vs. 73.1% of cases in male patients, respectively; Pearson χ2 test, p<0.001).
Source Investigation
A total of 3,035 potential sources were identified for the 1,991 reported LD cases (mean of 1.5 [SD 1.0] potential sources per patient). Technical Appendix 2 Table 1 shows the distribution of the different types of reported sources. Using the NLODP sampling criteria, the LSIU sampled 1,418 unique potential sources (47% of 3,035 reported sources). Some sources were sampled >1 time, resulting in 1,484 source investigations performed during the study period. In 367 (24.7%) of these investigations, Legionella spp. were identified in >1 sample, but large variations were seen among the different source types (Table 3). In 30 investigations, >1 Legionella spp. was found, identified as L. pneumophila SG1 or L. pneumophila non-SG1 if no L. pneumophila SG1 was found (Table 3). The proportions before and after introduction of the 4 criteria for sampling on June 1, 2006, were similar: 24.6% vs. 25.2%, respectively.
L. pneumophila SG1 was found in 97 (6.5%) investigations, L. pneumophila non-SG1 in 76 (5.1%), and Legionella spp. other than L. pneumophila in 194 (13.1%) (Table 3). The proportion of investigations in which L. pneumophila SG1 was found showed large variations among source types (Table 3). For instance, L. pneumophila SG1 was often detected in wellness centers (i.e., facilities offering spas, saunas, fitness equipment, massages, etc.) (40.5%); hospitals and health care settings (25.6%); and cooling towers (20.9%). However, L. pneumophila SG1 was not detected in investigated campsites, car wash or gasoline stations, or decorative water fountains and was detected in only a small proportion of investigated garden centers (1.2%). Residences were the most frequently sampled sources (51.3% of investigations); L. pneumophila SG1 was found in 21 (2.8%) of the 762 investigated residences (Table 3). Exclusion of source investigation data for the 119 nosocomial cases did not markedly change these results (Technical Appendix 2 Table 2).
Clusters
The cluster definition used by NLODP resulted in 105 identified clusters, of which 98 (93.3%) were location clusters and 7 (6.7%) were geographic clusters. These clusters involved 266 patients with LD (Table 4; Technical Appendix 2 Figure). An average of 2.9 (range 2–11) patients with LD were associated with each cluster (some patients were part of multiple clusters). In 50 clusters (47.6%), patients from >1 MHS were involved. Garden centers were the most frequently identified cluster site (27 [25.7%] clusters), followed by hospitals and health care settings (17 [16.2%] clusters), residences (10 [9.5%] clusters), wellness centers (9 [8.6%] clusters), and hotels (7 [6.7%] clusters) (Table 5). For the 98 location clusters, 142 source investigations were performed (23 cluster locations were investigated >1 time during the study period). Legionella spp. were found in 56 (39.4%) of investigations. L. pneumophila SG1 was found in 28 (19.7%) investigations, L. pneumophila non-SG1 in 6 (4.2%), and Legionella spp. other than L. pneumophila in 22 (15.5%).
Strain Characteristics
For the 1,991 reported patients with LD, 392 clinical isolates of Legionella spp. (85% of 460 reported patients diagnosed by culture) were sent to LSIU by the participating microbiologic laboratories in the Netherlands. All L. pneumophila SG1 clinical isolates and environmental strains were genotyped by using sequence-based typing (10–12), and monoclonal antibody determination was performed (13) (Technical Appendix 2 Tables 3, 4).
Matches
For the 392 patients with LD for whom a clinical isolate was available, 704 unique potential sources of investigation were identified (mean 1.8 [SD 1.2] sources per patient). For these sources, 478 investigations were performed, and Legionella spp. were found in a sample from 120 (25.1%) investigations.
Environmental strains were compared with the clinical isolate(s) from the patients associated with the sampled potential sources. During August 2002–August 2012, a total of 38 genotype matches were found for 41 patients with LD (3 matches involved 2 clinical isolates, and 35 matches involved 1 clinical isolate). For each patient with an isolate that was part of a genotype match, a mean of 1.9 (SD 1.6) potential sources of infection was identified. This mean was significantly higher than the mean 1.5 (SD 1.0) sources identified for patients whose clinical isolate could not be matched with an environmental strain (independent samples t-test, p<0.01). Table 6 shows the different types of sources from which the matching environmental strains were isolated. Most matches (15 [39%]) were with strains from hospitals or other health care settings, followed by those from residences (7 [18%]). A genotype match was found for 38 (31.7%) of 120 available clinical isolates that could be compared with an environmental strain (Technical Appendix 2 Table 5). For the 266 patients who were part of a cluster, 24 had clinical isolates that could be genotypically compared with environmental strains, and a genotype match occurred for 19 (79.2%) of these 24 patients.
During 2002–2012, a total of 1,991 patients with LD were reported in the Netherlands, and 1,484 source investigations were performed; 367 (24.7%) of the sources investigated were positive for Legionella spp. A total of 105 clusters were identified among 266 patients with LD. For 41 patients, a genotype match was found between the patient isolate and an environmental strain.
More than half of all source investigations were performed in residences, but only 20% of these investigations were positive for Legionella spp.; residences ranked tenth on the list of source types. A total of 43 cooling towers were investigated, ranking them third on the list of source types; >40% of those investigations were positive for Legionella spp. This well-known source of LD outbreaks should be considered often during source identification and investigation efforts performed by the MHS and LSIU.
For each patient, a mean of 1.5 potential sources of infection were reported, and about half of the reported sources were sampled. Although several attributes are being used by the MHS to improve source investigation (e.g., an elaborate questionnaire and a geographic information system implemented in 2009 [https://lpgis.geoxplore.nl/webify/?app=lpgis_ggd]), the number of sources being sampled could be increased. When the genotypic matches were analyzed, the mean number of sources identified and investigated for the patients involved was considerably higher (1.9 sources per patient), suggesting that identification and investigation of more potential sources of infection by the MHS may increase the proportion of patients with LD for whom a likely source of infection can be established.
Garden centers ranked third (after residences and workplaces) on the list of the most frequently reported potential sources of LD infection; 26% of identified clusters were associated with a garden center, indicating that this source type is often visited by patients with LD during the 2–14 days before symptom onset. However, only 8 of 86 investigated garden centers were found positive for Legionella spp. during source investigations. Several studies have shown the presence of Legionella spp. in potting soil samples (14–16), and the use of amebal coculture techniques has shown promising results in recovering L. pneumophila SG1 sequence type (ST) 46 (the third most frequently found ST in clinical isolates) from samples with a high likelihood of microbial flora (17). At this time, potting soil samples collected by NLODP are not regularly being investigated by the amebal coculture technique. These findings suggest that potting soil samples from garden centers identified as potential sources of infection for patients with LD should be examined closely.
Notwithstanding the extensive efforts by NLODP collaborators, the number of L. pneumophila SG1 strains that could be derived from investigated potential sources was relatively low (114 strains over 10 years). Despite systematic methods of source identification by using a standardized questionnaire covering >20 source types, a source could not be confirmed in most cases. Although the questionnaire is regularly evaluated and adjusted on the basis of new insights concerning reported sources of infection, it primarily covers sources identified from the literature, possibly explaining the low success rate; actual sources of infection may not be captured in the questionnaire. This hypothesis is supported by the differences in genotype variation between clinical isolates and environmental strains: one third of all culture-positive patients with LD were infected by L. pneumophila SG1 ST47, a rare finding in environmental samples.
The experiences of NLODP show the importance of organizing a multidisciplinary collaboration in which MHSs, treating physicians, and microbiologic laboratories are represented and aware of the importance of different aspects of surveillance and source investigation for patients with LD. Our findings show the necessity of increasing awareness among various groups: physicians for diagnosis of LD, MHSs for extensive source identification, and laboratories for performance of adequate diagnostics and collection of clinical and environmental isolates. During 2002–2012, the number of reported patients with LD and the number of identified clusters of patients did not change dramatically, which may suggest the limited effects of NLODP. However, one could argue that this relatively stable number of patients with LD could have resulted from the program. Despite the rational, systematic approach used by NLODP during this decade, most sources of LD infections went undiscovered, stressing the need for evaluating other, yet unknown, potential sources of infection. Also, a need exists for further investment in improving laboratory techniques for detection of Legionella spp. in samples with a high background of microbial flora such as soil.
Dr. Den Boer is a public health physician and epidemiologist at the Regional Public Health Laboratory Kennemerland, Haarlem, the Netherlands. His research interests include prevention and control of infectious diseases.
Acknowledgment
We thank the public health physicians and nurses of the MHSs for providing epidemiologic data and source identification results; the treating physicians and microbiologists for making patient isolates available for genotyping; and Jacqueline De Vries and Wim Houtenbos for their support with source investigations.
References
- Fields BS, Benson RF, Besser RE. Legionella and Legionnaires’ disease: 25 years of investigation. Clin Microbiol Rev. 2002;15:506–26. DOIPubMedGoogle Scholar
- Torres A, Blasi F, Peetermans WE, Viegi G, Welte T. The aetiology and antibiotic management of community-acquired pneumonia in adults in Europe: a literature review. Eur J Clin Microbiol Infect Dis. 2014;33:1065–79. DOIPubMedGoogle Scholar
- Joseph CA, Ricketts KD. Legionnaires’ disease in Europe 2007–2008. Euro Surveill. 2010;15:19493.PubMedGoogle Scholar
- Beauté J, Zucs P, de Jong B; European Legionnaires’ Disease Surveillance Network. Legionnaires disease in Europe, 2009–2010. Euro Surveill. 2013;18:20417.PubMedGoogle Scholar
- Den Boer JW, Yzerman EP, Schellekens J, Lettinga KD, Boshuizen HC, Van Steenbergen JE, A large outbreak of Legionnaires' disease at a flower show, the Netherlands, 1999. Emerg Infect Dis. 2002;8:37–43. DOIPubMedGoogle Scholar
- Netherlands Ministry of Housing, Spatial Planning and the Environment. Water supply decree. Besluit van 26/10/2004 to wijziging van het Waterleidingbesluit en het Besluithygiëne en veiligheid badinrichtingen en zwemgelegenheden (preventie van legionella in leidingwater). The Hague (the Netherlands): the Ministry; 2004.
- Sonder GJ, van den Hoek JA, Bovée LP, Aanhane FE, Worp J, De Ry van Beest Holle M, Changes in prevention and outbreak management of Legionnaires’ disease in the Netherlands between two large outbreaks in 1999 and 2006. Euro Surveill. 2008;13:18983.PubMedGoogle Scholar
- Den Boer JW, Verhoef L, Bencini MA, Bruin JP, Jansen R, Yzerman EP. Outbreak detection and secondary prevention of Legionnaires’ disease: a national approach. Int J Hyg Environ Health. 2007;210:1–7. DOIPubMedGoogle Scholar
- Bhopal RS. Geographical variation of Legionnaires’ disease: a critique and guide to future research. Int J Epidemiol. 1993;22:1127–36. DOIPubMedGoogle Scholar
- Fry NK, Bangsborg JM, Bernander S, Etienne J, Forsblom B, Gaia V, Assessment of intercentre reproducibility and epidemiological concordance of Legionella pneumophila serogroup 1 genotyping by amplified fragment length polymorphism analysis. Eur J Clin Microbiol Infect Dis. 2000;19:773–80. DOIPubMedGoogle Scholar
- Gaia V, Fry NK, Afshar B, Lück PC, Meugnier H, Etienne J, Consensus sequence-based scheme for epidemiological typing of clinical and environmental isolates of Legionella pneumophila. J Clin Microbiol. 2005;43:2047–52. DOIPubMedGoogle Scholar
- Ratzow S, Gaia V, Helbig JH, Fry NK, Lück PC. Addition of neuA, the gene encoding N-acylneuraminate cytidylyl transferase, increases the discriminatory ability of the consensus sequence-based scheme for typing Legionella pneumophila serogroup 1 strains. J Clin Microbiol. 2007;45:1965–8. DOIPubMedGoogle Scholar
- Helbig JH, Bernander S, Castellani Pastoris M, Etienne J, Gaia V, Lauwers S, Pan-European study on culture-proven Legionnaires’ disease: distribution of Legionella pneumophila serogroups and monoclonal subgroups. Eur J Clin Microbiol Infect Dis. 2002;21:710–6. DOIPubMedGoogle Scholar
- Koide M, Saito A, Okazaki M, Umeda B, Benson RF. Isolation of Legionella longbeachae serogroup 1 from potting soils in Japan. Clin Infect Dis. 1999;29:943–4. DOIPubMedGoogle Scholar
- Steele TW, Lanser J, Sangster N. Isolation of Legionella longbeachae serogroup 1 from potting mixes. Appl Environ Microbiol. 1990;56:49–53.PubMedGoogle Scholar
- Casati S, Gioria-Martinoni A, Gaia V. Commercial potting soils as an alternative infection source of Legionella pneumophila and other Legionella species in Switzerland. Clin Microbiol Infect. 2009;15:571–5. DOIPubMedGoogle Scholar
- Schalk JA, Docters van Leeuwen AE, Lodder WJ, De Man H, Euser SM, Den Boer JW, Isolation of Legionella pneumophila from pluvial floods by amoebal coculture. Appl Environ Microbiol. 2012;78:4519–21. DOIPubMedGoogle Scholar
Figure
Tables
Cite This ArticleTable of Contents – Volume 21, Number 7—July 2015
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Jeroen W. Den Boer, Regional Public Health Laboratory Kennemerland, Boerhaavelaan 26, 2035 RC, Haarlem, the Netherlands
Top