Volume 20, Number 8—August 2014
Dispatch
New Introductions of Enterovirus 71 Subgenogroup C4 Strains, France, 2012
Abstract
In France during 2012, human enterovirus 71 (EV-A71) subgenogroup C4 strains were detected in 4 children hospitalized for neonatal fever or meningitis. Phylogenetic analysis showed novel and independent EV-A71 introductions, presumably from China, and suggested circulation of C4 strains throughout France. This observation emphasizes the need for monitoring EV-A71 infections in Europe.
Human enterovirus 71 (EV-A71) is a member of the enterovirus species A in the family Picornaviridae, genus Enterovirus. On the basis of the 1D gene sequences encoding the VP1 capsid protein (1DVP1), EV-A71 has been classified into 3 genogroups (A–C) and 12 subgenogroups (A, B0–B5, C1–C5) (1); in addition, 3 new genogroups (D–F) were recently identified (2–4). In children, EV-A71 mainly causes asymptomatic or benign infections, such as neonatal fever and hand-foot and mouth disease (HFMD); less frequently, EV-A71 causes neurologic complications, such as encephalitis and poliomyelitis-like paralysis (1).
In the Asia–Pacific region, EV-A71 has emerged as a major public health concern over the past 15 years. Large outbreaks have been reported, associated with the emergence of new genogroups and subgenogroups, high rates of illness, and fatal cases of encephalitis (1,5). The largest epidemic expansion of EV-A71 occurred in China, mainly caused by EV-A71 subgenogroup C4 (EV-A71 C4) strains (5,6). By contrast, epidemic activity is low in Europe, where only 4 outbreaks of EV-A71 infection have been reported over the past 40 years: Bulgaria (1975), Hungary (1978), and the Netherlands (1986, 2007) (5,7). Most of the cases of EV-A71 infection reported since 1986 have been caused by subgenogroup C1 and C2 strains (7–9). In 2004, EV-A71 C4 strains were rarely detected in France, Germany, and Austria (8–11), and no other EV-A71 C4 cases were reported in Europe until 2012, when we detected C4 strains in 4 hospitalized patients, suggesting that dissemination of the C4 strains was restricted during 2004–2011. We describe the clinical cases caused by the EV-A71 C4 strains detected in 2012 and address the origin of these newly detected viruses.
In France, EV infections diagnosed in hospital settings have been voluntarily reported to the National Institute for Public Health by a network of hospital laboratories since 2000 (9). In 2012, a total of 2,088 EV infections were reported by the laboratory network. In addition, in 2010, a total of 158 community cases of HFMD and herpangina were reported through a sentinel surveillance system implemented in Clermont-Ferrand, France (12). As part of the national surveillance, 1,249 EV strains were analyzed by 6 laboratories in the EV network (including the 2 National Enterovirus Reference Center laboratories in Lyon and Clermont-Ferrand). Of the 1,249 EV strains, 1,105 (88.5%) were successfully genotyped. Most of the genotyped strains were detected in cerebrospinal fluid (CSF) samples from patients with neonatal fever, meningitis, or meningoencephalitis or in samples from patients with HFMD or herpangina. Of the 1,105 genotyped EV strains, 16 (1.4%) were EV-A71 strains. Among these 16 cases of EV-A71 infection, a fatal case of rhomboencephalitis was diagnosed in an adult who had been treated with rituximab (13). On the basis of the complete 1D gene sequences encoding the VP1 capsid protein (1DVP1), 12 of the 16 EV-A71 strains were assigned to subgenogroup C2, and 4 were assigned to subgenogroup C4.
We conducted a retrospective review of medical records for the 4 patients with EV-A71 C4 infection to document the patients’ ages at diagnosis, clinical symptoms, length of hospitalization, and laboratory findings. The EV-A71 C4 infections were detected throughout the year in 3 regions (Brittany, Ile de France, and Provence-Alpes-Côte d’Azur). Of the 4 patients, 3 (6, 17, and 21 days of age) had neonatal fever when medical care was sought, and 1 patient (4 years of age) had meningitis (Table). The 21-day-old infant had persisting irritability and was hospitalized for 6 days. No severe neurologic complications were observed, and all 4 children had a favorable outcome. Bacterial culture results for CSF, blood, and urine samples from all 4 children were negative, and molecular detection results for herpes simplex virus types 1 and 2 and varicella-zoster virus in CSF were also negative. For the 3 children with neonatal fever, reverse transcription PCR was positive for EV-A71 in CSF specimens. For the child with meningitis, reverse transcription PCR was negative for EV-A71 in the CSF specimen, but an EV-A71 strain was isolated from a throat swab specimen.
Figure
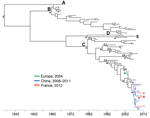
Figure. Dated phylogeny inferred by using 97 enterovirus 71 (EV-A71) 1D gene sequences encoding the VP1 capsid proteins (1DVP1)The dataset included the 4 sequences determined in this study; 37 sequences from EV-A71...
Phylogenetic analyses based on a Bayesian approach were performed with a set of 97 1DVP1 sequences (Figure; Technical Appendix). The chronogram clearly shows that the EV-A71 C4 strains detected in France in 2012 (Figure, red branches) and those detected in France, Austria, and Germany in 2004 (Figure, green branches) belong to 2 separate lineages. The 4 strains detected in 2012 in France clustered with EV-A71 C4 strains detected in China during 2008–2011. We estimated that the most recent common ancestor of this cluster (Figure, blue branches) emerged, presumably in China, during 2006 (95% highest posterior density interval 2005–2007). Of the 4 EV-A71 C4 strains detected within a 4-month period in geographically distant (≈1,100 km) French regions, 2 displayed direct clustering (posterior probability 0.999) but substantial variation (genetic distance of 0.018 nt substitution per site between the corresponding 1DVP1 sequences). The quick evolution of the 2 EV-A71 C4 strains from their common ancestor suggests local spread of the viruses. The other 2 strains displayed consistent clustering (posterior probability >0.8) with different strains isolated in China, suggesting independent introductions of virus.
In 2012, EV-A71 C4 strains were detected in France in 4 children hospitalized for neonatal fever or meningitis. Although EV-A71 C4 strains have circulated extensively in China since 2008, this virus has rarely been detected in Europe. In France, 133 cases of EV-A71 infections were reported during January 2000–May 2013 (9) (I. Schuffenecker, unpub. data). EV-A71 C2 infections have been predominant since 2007; however, only 5 cases of EV-A71 C4 infection have been identified in the country since 2004. Our Bayesian analyses excluded a direct evolution of the 2012 EV-A71 C4 strains from the earlier 2004 European virus lineage. The phylogenetic data are consistent with 3 independent virus introductions, presumably from China, and are compatible with a more global circulation of subgenogroup C4 enteroviruses. In 2013, the C4 subgenogroup also emerged in Russia, where it was associated with an outbreak of 78 reported cases, including 1 fatal case of meningoencephalitis (14).
Many cases of fatal encephalitis have been associated with EV-A71 C4 infection outbreaks in China (6), which highlights the neurovirulence of EV-A71 strains. Rare acute flaccid paralysis cases have also been reported in Australia through the national poliomyelitis surveillance program (15). Although the prevalence of neurologic cases associated with EV-A71 infection is currently low in Europe, the recent circulation of EV-A71 C4 in France and in Rostov, Russia (along the eastern border with Europe), underscores the need for improved surveillance of neurologic manifestations associated with EV infection and of the incidence of HFMD within communities. In addition, careful monitoring for the possible introduction and circulation of new EV-A71 genogroups and subgenogroups should be conducted.
Dr Schuffenecker is a virologist working at the National Reference Center for Enterovirus and Parechovirus. She is involved in diagnosis and surveillance of enterovirus and parechovirus infections.
Acknowledgment
We are grateful to Laurence Josset for critical review of the manuscript and revision of the English. We also acknowledge Delphine Falcon and Katy Pinet for their technical contributions.
References
- Solomon T, Lewthwaite P, Perera D, Cardosa MJ, McMinn P, Ooi MH. Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect Dis. 2010;10:778–90. DOIPubMedGoogle Scholar
- Deshpande JM, Nadkarni SS, Francis PP. Enterovirus 71 isolated from a case of acute flaccid paralysis in India represents a new genotype. Curr Sci. 2003;84:1350–3.
- Bessaud M, Pillet S, Ibrahim W, Joffret ML, Pozzetto B, Delpeyroux F, Molecular characterization of human enteroviruses in the Central African Republic: uncovering of wide diversity and identification of a new human enterovirus A71 genogroup. J Clin Microbiol. 2012;50:1650–8. DOIPubMedGoogle Scholar
- Bessaud M, Razafindratsimandresy R, Nougairede A, Joffret ML, Deshpande JM, Dubot-Peres A, Molecular comparison and evolutionary analyses of VP1 nucleotide sequences of new African human enterovirus 71 isolates reveal a wide genetic diversity. PLoS ONE. 2014;9:e90624. DOIPubMedGoogle Scholar
- Yip CCY, Lau SKP, Woo PCY, Yuen K-Y. Human enterovirus 71 epidemics: what’s next? Emerg Health Threats J. 2013;6:19780–97.
- Zhang Y, Tan X, Cui A, Mao N, Xu S, Zhu Z, Complete genome analysis of the C4 subgenotype strains of enterovirus 71: predominant recombination C4 viruses circulating in China for 14 years. PLoS ONE. 2013;8:e56341. DOIPubMedGoogle Scholar
- van der Sanden S, van der Avoort H, Lemey P, Uslu G, Koopmans M. Evolutionary trajectory of the VP1 gene of human enterovirus 71 genogroup B and C viruses. J Gen Virol. 2010;91:1949–58. DOIPubMedGoogle Scholar
- Mirand A, Schuffenecker I, Henquell C, Billaud G, Jugie G, Falcon D, Phylogenetic evidence for a recent spread of two populations of human enterovirus 71 in European countries. J Gen Virol. 2010;91:2263–77. DOIPubMedGoogle Scholar
- Schuffenecker I, Mirand A, Antona D, Henquell C, Chomel JJ, Archimbaud C, Epidemiology of human enterovirus 71 infections in France, 2000–2009. J Clin Virol. 2011;50:50–6. DOIPubMedGoogle Scholar
- Ortner B, Huang CW, Schmid D, Mutz I, Wewalka G, Allerberger F, Epidemiology of enterovirus types causing neurological diseases in Austria 1999–2007: detection of clusters of echovirus 30 and enterovirus 71 and analysis of prevalent genotypes. J Med Virol. 2009;81:317–24. DOIPubMedGoogle Scholar
- Diedrich S, Weinbrecht A, Schreier E. Seroprevalence and molecular epidemiology of enterovirus 71 in Germany. Arch Virol. 2009;154:1139–42 and. DOIPubMedGoogle Scholar
- Mirand A, Henquell C, Archimbaud C, Ughetto S, Antona D, Bailly J-L, Outbreak of hand, foot and mouth disease/ herpangina associated with coxsackievirus A6 and A10 infections in 2010, France: a large citywide, prospective observational study. Clin Microbiol Infect. 2012;18:E110–8. DOIPubMedGoogle Scholar
- Kassab S, Saghi T, Boyer A, Lafon M-E, Gruson D, Lina B, A fatal case of enterovirus 71 infection complicating rituximab therapy, France, 2012. Emerg Infect Dis. 2013;19:1345–7. DOIPubMedGoogle Scholar
- Akhmadishina LV, Eremeeva TP, Trotsenko OE, Ivanova OE, Mikhailov MI, Lukashev AN. Seroepidemiology and molecular epidemiology of enterovirus 71 in Russia. PLoS ONE. 2014;9:e97404. DOIPubMedGoogle Scholar
- Thorley B. Detection of enterovirus 71 sub-genogroup C4a in specimens from cases of acute flaccid paralysis, Australia. ProMed. 2013 May 26 [cited 2013 Dec 1]. http://www.promedmail.org, archive no. 20130526.1738087.
Figure
Table
Cite This ArticleTable of Contents – Volume 20, Number 8—August 2014
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Isabelle Schuffenecker, Centre National de Référence des Enterovirus et Parechovirus, Laboratoire de Virologie, Groupement Hospitalier Est, 59 Bd Pinel, 69677 Bron, France
Top